

A tablet that releases its drug over eight hours instead of two is not just a convenience. It maintains a more stable concentration in the bloodstream, reduces the number of doses a patient has to remember, and can avoid the peaks that cause side effects and the troughs that cause therapeutic failure. Modified-release technology makes this possible by controlling not just how much drug is delivered, but when, where, and at what rate.
This article explains the main mechanisms used in modified-release oral solid dosage forms, the excipients that make them work, and the formulation logic behind each approach. It is written for pharmaceutical professionals who need a clear working understanding of the science rather than a textbook-level deep dive.
What "modified release" actually means
The term covers any oral dosage form where the rate, timing, or location of drug release has been deliberately altered from what would happen if the drug were simply compressed into a tablet with no release-controlling technology. Regulatory frameworks split this into two main categories:
- Extended release (ER/SR): the drug is released more slowly than from an immediate-release formulation, typically over 8 to 24 hours, maintaining therapeutic plasma concentrations with less frequent dosing.
- Delayed release (DR): the drug is held back entirely until the tablet reaches a specific part of the gastrointestinal tract, usually the small intestine, and then released. Enteric-coated tablets fall in this category.
Some formulations combine both: a delayed start followed by extended delivery once release begins.
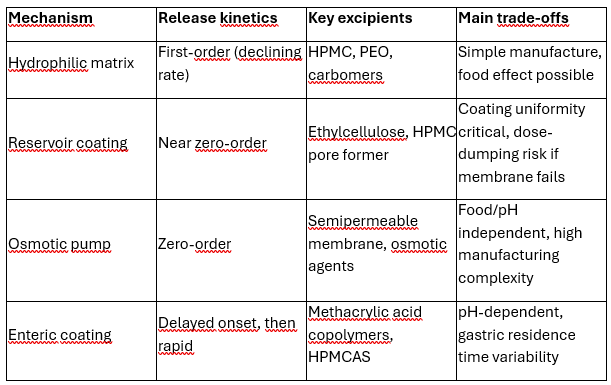
Mechanism 1: Hydrophilic matrix tablets
The hydrophilic matrix is the most widely used extended-release technology in oral solid dosage forms. It works through a sequence of physical events that unfold as the tablet passes through the gastrointestinal tract.
When the tablet contacts gastrointestinal fluid, the hydrophilic polymer on its surface begins to absorb water and swell. This creates a viscous gel layer around the tablet core, which acts as a physical barrier between the drug inside and the fluid outside. The gel layer does not block drug release — it controls the rate at which it happens.
As PMC research on HPMC matrix erosion in vivo describes: water diffuses inward, causing the HPMC matrix to swell and form a rubbery gel. Soluble drugs diffuse outward through the gel layer; poorly soluble drugs are released mainly as the gel erodes at its outer surface. Most real formulations involve both mechanisms simultaneously, with the balance determined by drug solubility and polymer concentration.
The role of HPMC
Hydroxypropyl methylcellulose (HPMC, also called hypromellose) is the dominant polymer in hydrophilic matrix formulations. Its dominance comes from a combination of properties that are difficult to find together: it hydrates rapidly on contact with water, forms a coherent and resilient gel, is compatible with a wide range of drugs, and has a well-established safety and regulatory profile.
As a comprehensive review on HPMC as a pharmaceutical excipient documents, drug release from HPMC matrices occurs by two routes: diffusion of molecules through the gel layer, and progressive degradation of the polymer matrix at the dissolution front. Highly water-soluble drugs follow predominantly diffusion kinetics; poorly soluble drugs are released mainly by erosion.
The viscosity grade of HPMC controls how thick and resilient the gel layer becomes, which in turn controls how slowly drug diffuses through it. Higher viscosity grades (K15M, K100M) form thicker, more robust gels that sustain drug release longer. Lower viscosity grades produce thinner gels that erode more quickly, giving faster release profiles. As gel strength studies on commercial matrix tablets demonstrate, tablets formulated with HPMC K15M or K100M showed gel strengths above 0.02 MPa and predominantly diffusion-controlled release, while lower-viscosity grades shifted toward erosion-controlled kinetics.
Other hydrophilic matrix polymers
Polyethylene oxide (PEO) is used as an alternative to HPMC, particularly for high drug-loading applications. It forms gels with similar controlled-release behaviour, but its sensitivity to thermal oxidation requires careful management of processing conditions and storage. Studies on PEO matrix tablets confirm that drug release is affected by storage time, polymer molecular weight, and drug solubility — all factors that need to be addressed during formulation development.
Carbomers, carrageenan, xanthan gum, and various cellulose derivatives are also used, often in combination with HPMC to modify release kinetics or improve robustness.
Mechanism 2: Reservoir systems
In a reservoir system, the drug core is surrounded by a rate-controlling membrane. Drug dissolves from the core, diffuses through the membrane, and is released at a rate governed by the membrane's permeability and thickness.
Unlike a matrix system — where the geometry changes as the tablet erodes and the drug concentration in the matrix falls — a well-designed reservoir system can maintain a nearly constant concentration gradient across the membrane for most of the dose duration. This produces closer to zero-order release kinetics, meaning the drug is delivered at a roughly constant rate rather than declining over time.
Membrane materials include ethylcellulose (water-insoluble, used as the primary rate-controlling polymer), combined with water-soluble pore formers such as HPMC or polyethylene glycol. As the tablet dissolves in gastrointestinal fluid, the water-soluble component leaches out of the membrane, creating channels through which drug can diffuse. The ratio of water-insoluble to water-soluble polymer in the coating controls the effective porosity and thus the release rate.
Why reservoir systems are more complex to manufacture
The membrane must be applied uniformly over the entire tablet surface. Non-uniformity in coating thickness creates localised high-permeability zones that produce premature drug release. Film-coated tablets and coated multiparticulate systems (pellets, granules in capsules) both use reservoir principles, but multiparticulates are generally more robust to coating variability because each unit is small and the population average governs the release profile.
Mechanism 3: Osmotic pump systems
Osmotic systems control drug delivery through osmotic pressure rather than diffusion or erosion. The tablet core is surrounded by a semipermeable membrane — permeable to water but not to drug or osmotic agents — with a small laser-drilled orifice. As a comprehensive review of osmotic pump drug delivery describes, water enters through the semipermeable membrane driven by the osmotic pressure difference between the core and the surrounding fluid. The dissolved or suspended drug is then pushed out through the orifice at a rate controlled by the rate of water ingress.
The key advantage of osmotic systems is that the release rate is essentially independent of the gastrointestinal environment — pH, motility, and fed versus fasted state have minimal effect, because the driving force is the osmotic pressure gradient rather than the local fluid conditions. This makes osmotic systems attractive for drugs where consistent systemic exposure is critical.
The most common design is the push-pull osmotic tablet, which contains two layers: an active layer with the drug and osmotic excipients, and a push layer containing an expanding osmotic agent. As water enters, the push layer expands and drives drug out of the orifice at a controlled rate. The rate can be adjusted by changing the orifice diameter, membrane thickness, and osmotic agent loading.
Osmotic systems are more expensive to manufacture than matrix tablets, requiring precision drilling of the delivery orifice and consistent semipermeable membrane application. They are used when the pharmacokinetic requirements are stringent and the drug cannot be adequately controlled by simpler technologies.
Mechanism 4: Enteric-delayed release
Enteric coatings are applied to tablets when the drug must not be released in the stomach — either because the drug is destroyed by gastric acid, because the drug irritates the gastric mucosa, or because release is intended for the colon or small intestine.
The coating material is an acid-insoluble polymer that remains intact at the low pH of the stomach (approximately pH 1 to 2) and dissolves when the tablet reaches the higher pH environment of the small intestine (approximately pH 5.5 to 7). As PMC research on enteric-coated HPMC capsules explains: in acidic gastric media, the enteric polymer is protonated and therefore insoluble; with increasing pH and bicarbonate concentration along the intestine, the polymer becomes ionised and water-soluble, allowing drug release to begin.
Common enteric polymers include:
- Methacrylic acid copolymers (various grades, dissolving at pH thresholds between 5.5 and 7.0)
- Hypromellose acetate succinate (HPMCAS)
- Hypromellose phthalate (HPMCP)
- Cellulose acetate phthalate (CAP)
The specific pH at which dissolution begins depends on the polymer grade. This allows formulators to target release to different regions of the gastrointestinal tract: early small intestine for maximum absorption, or distal small intestine and colon for local action in inflammatory bowel disease or colon-targeted delivery.
Enteric coatings are also used to protect amorphous solid dispersions from the gastric environment, where crystallisation of an amorphous drug can compromise bioavailability. As research on enteric-coated amorphous solid dispersions shows, the coating can protect against drug crystallisation during gastric transit and maintain the dissolution advantage of the amorphous form.
How release mechanism affects formulation choices
The choice of mechanism is not purely technical — it shapes every downstream decision in formulation development.
Drug solubility is the first filter. Highly water-soluble drugs release rapidly from hydrophilic matrices by diffusion and are difficult to slow; they are often better controlled by reservoir or osmotic systems. Poorly soluble drugs release mainly by erosion from hydrophilic matrices, which is easier to control but can show food effects due to bile salt-enhanced dissolution.
Drug dose is the second filter. High-dose drugs require excipients that can accommodate them at reasonable tablet size. Hydrophilic matrix systems can typically handle up to 80% drug by weight if the polymer is compatible; reservoir and osmotic systems impose tighter constraints because the coating must remain functional regardless of tablet geometry.
The food effect problem
All extended-release tablet technologies are susceptible to food effects to varying degrees, because food alters gastric pH, motility, emptying rate, and bile salt concentration. Fatty meals slow gastric emptying and can change the hydrodynamic environment around a dissolving matrix tablet. High-calorie meals can accelerate drug release from certain lipid-based systems.
The most serious food effect is dose dumping: rapid, uncontrolled release of the entire drug content from a modified-release formulation in the presence of food or alcohol. This is a particular risk for reservoir systems where the membrane is disrupted by high ethanol concentrations. Regulatory guidance from the FDA and EMA requires food-effect studies for all modified-release products, and the label must specify whether the product should be taken with or without food.
Osmotic systems are the most food-independent of the common technologies, which is part of their value for narrow-therapeutic-index drugs.
Testing modified-release tablets: dissolution
Dissolution testing is the primary in vitro tool for characterising modified-release performance and verifying batch-to-batch consistency. For extended-release tablets, the test runs over the intended release period (typically 8 to 24 hours) and measures the fraction of drug released at multiple timepoints. The specification typically requires release within defined windows at each timepoint — for example, 20 to 40% at 2 hours, 45 to 65% at 6 hours, and not less than 80% at 12 hours.
For enteric-coated tablets, the dissolution method includes an acid stage (pH 1.0 to 1.2, simulating the stomach) followed by a buffer stage (pH 6.8 or higher, simulating the intestine). The specification requires minimal release during the acid stage (typically less than 10% in 2 hours) and adequate release during the buffer stage.
Dissolution testing is a surrogate for in vivo performance, and the relationship between dissolution and bioavailability — the in vitro/in vivo correlation (IVIVC) — is sought during development to allow dissolution data to predict clinical pharmacokinetics. A validated IVIVC can reduce the number of clinical studies required during product development and post-approval changes.
FAQ
Why can't you crush a modified-release tablet?
Crushing destroys the release-controlling architecture — whether it is the gel-forming matrix, the reservoir membrane, or the enteric coating. The entire dose is then available for immediate absorption, which can produce toxic plasma concentrations for drugs with narrow therapeutic windows. Some modified-release tablets contain extended-release granules in a conventional tablet matrix and can be split without destroying release control, but this must be confirmed product by product.
What is the difference between ER, SR, XR, and CR on a drug name?
These suffixes — extended release, sustained release, extended release, and controlled release respectively — describe the same general category of technology: drug delivery that extends the release profile beyond immediate release. The specific mechanism differs by product. The naming convention varies by manufacturer and regulatory region, not by mechanism.
Can any drug be made into a modified-release tablet?
Not readily. Drugs with very short half-lives relative to transit time (gastric plus intestinal, typically 12 to 24 hours) are good candidates because extending release maintains plasma concentrations. Drugs with very long half-lives already provide sustained exposure from immediate-release dosing and gain little from modified-release technology. Drugs absorbed only in a narrow window of the gastrointestinal tract (absorption window drugs) present a specific challenge: extended release may carry the drug past the absorption site before it is released.
What causes the "dose dumping" risk in modified-release products?
Dose dumping occurs when the release-controlling mechanism fails and the entire drug content is released at once. The most common causes are: physical damage to a reservoir coating (from chewing, crushing, or high-alcohol conditions), failure of a polymer matrix under extreme hydrodynamic conditions, or a defective enteric coating that does not provide adequate acid protection. FDA guidance requires in vitro testing with ethanol to screen for alcohol-induced dose dumping.
How does the choice of polymer grade affect release rate in HPMC matrices?
Higher viscosity grades of HPMC form thicker, more resilient gel layers on contact with water. This increases the diffusion path length for drug molecules and slows their release rate. Lower viscosity grades form thinner gels that erode more rapidly, giving faster release. Within a given grade, increasing HPMC concentration also slows release by increasing gel viscosity and reducing effective drug diffusivity through the matrix.